Features
Continuing Education
Patient Care
“Sing” outside the box – laryngeal release and its practice success
January 11, 2022 By Cheryl Mazak, RMT
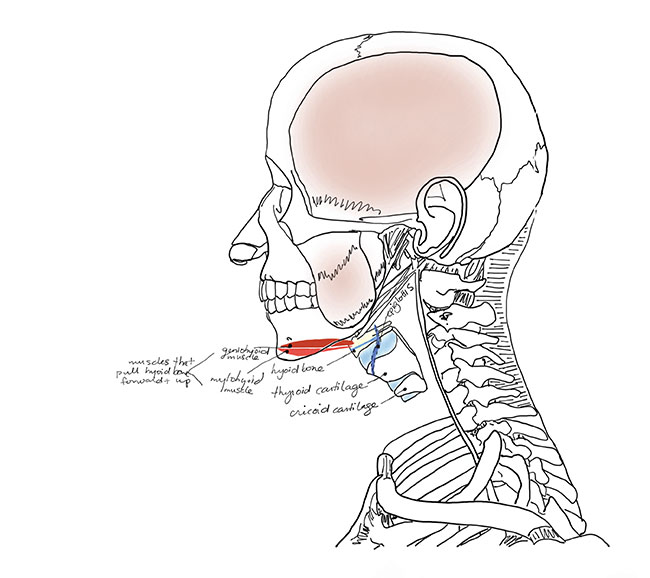 Muscles that pull the larynx anteriorly and superiorly during initiation of swallowing.
All images courtesy of the author.
Muscles that pull the larynx anteriorly and superiorly during initiation of swallowing.
All images courtesy of the author. Speech and swallowing weren’t on my radar at all. My goals were all about finding relief for the pain in my jaw – ways to decrease the pain and hypertonicity in my own TMJ.
I started taking a close look at every muscle that moves the jaw because working directly in the area of the temporomandibular joint itself only seemed to briefly dampen the pain, discomfort and tension. I began to palpate and thoroughly investigate the front of my neck (inferior to the mandible) and discovered that there was an incredible amount of hypertonicity in the suprahyoids and infrahyoids. After a thorough exploration and applying stretching to this musculature, I had the most relief I had ever felt in my TMJ – but it didn’t end there.
I noticed immediately after the first hour of treatment that I performed on myself that I was taking deeper breaths than I had been before treatment. Swallowing was occurring with less effort and my voice was more relaxed and lower in pitch. I figured those responses were due to being relaxed and pain-free for the first time in nearly a decade.
I had practiced regularly and developed new techniques to be able to reach these muscles: I found a way to safely grip and hang on to them so that I could change their length and soften their fibres through transverse stretching. The muscles responded favourably and began to lengthen. The position of my head and neck became more neutral and imbalances decreased.
I was starting to realize that there was a connection between speech, and swallowing strength and function through soft tissue work. I began to consult with several speech/language pathologists (SLPs), otolaryngologists (ENTs), dentists and physicians to discuss the relevancy of the extrinsic laryngeal muscles and their connection to speech and swallowing limitations.
This information is derived from data I’ve collected over the past six years working regularly and specifically with these treatments. My information stems from anecdotal evidence and individual case studies with volunteers, and countless hours of research and development and conferring with other HCP’s.
A thorough understanding
For the safe application of hyolaryngeal release, you need to develop an extensive knowledge of the anterior neck anatomy as well as the mechanics of speech, swallowing and respiration. A strong understanding of the mechanics of the functions in these systems is integral so that you fully understand what role each muscle plays in each individual function. With proper palpations and specific techniques, it has been proven to be very safe and effective within my case files.
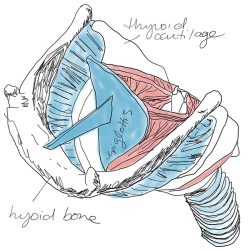
Position of epiglottis inside the larynx.
In general, the anterior neck muscles are important to address in most situations, especially in this age where our heads are forward flexed more than ever. If there is pain in the posterior neck, it can often be due to the anterior neck muscles becoming shortened. This puts an enormous strain on the posterior neck muscles which then have to work against gravity, force and weight while they are in a lengthened, forward flexed position.
The patient must be fully informed and be able to tolerate transverse stretching in the anterior neck for the treatments to be effective.
Just as important as understanding the possible positive outcomes when working in the anterior neck while addressing speech/swallowing conditions, knowing the limitations is equally important. In my practice, I have found that working on the suprahyoids and infrahyoids has had no effect on dampening issues such as spasmodic dysphonia and essential voice tremors. It is important to thoroughly discuss these limitations with your patient to provide realistic expectations. Knowing the conditions of speech and swallowing dysfunction is very important when addressing the muscles to treat speech and swallowing issues. As with any soft tissue approach, you will need to explain that there might be soreness post-treatment, but the benefits have always outweighed any post-treatment, temporary discomfort for my patients.
You need to have excellent palpation skills to perform this work as some of the muscles may be difficult to identify since they are layered so closely. Displacement of the hyoid and larynx is likely to appear when a patient presents with torticollis.
Along came a singer
I was presented with the file of a singer who needed treatment for their neck and TMJ following a motor vehicle accident. I decided that this was a good time to apply anterior neck and jaw treatment after having such success with my own jaw. It’s a very tiring treatment that requires a lot of focus by both the therapist and the patient with concentrated breathing by the patient to allow the muscles to release during the treatment.
After the treatment was completed, they remarked, “Wow, I feel like an alto.” This was very interesting because they are a soprano. I asked them to wait a few hours then sing and let me know what was experienced. They came back the following week and told me that they were singing alto notes that they had never been able to reach in their life. Although there was no gain at the top end of their pitch, the soprano notes were noticeably more effortless to sing and much smoother. They were not having to use as much force to sing the notes.
It was a very positive result and of course, this is where my interest in research and development really began for treatments aimed at speech and swallowing restrictions. When I was presented with my first patient with Parkinson’s, it was like the reasons for these treatments suddenly had a much larger purpose. I began to apply the treatments and incredible changes started to happen. I was very cautious to not over-promise any results. We kept the expectations reasonably low and were very pleasantly surprised. When a patient presented with vocal restrictions, like a forced whisper, they ended up having a smoother sound post-treatment with more clarity and projection, which was extremely exciting. According to the majority of my patient reporting, Parkinson’s medications had very little effect on preserving or improving the function of speech and swallowing. They seem to be most helpful with movement issues.
Aspiration pneumonia is still one of the most threatening dangers facing those with Parkinson’s. I started to hypothesize that perhaps the shortening of the anterior neck muscles is a physical response to the involuntary movements, tremors and bracing that a person does to prevent falling.

Hyoid bone and cartilages of the larynx visible from the exterior view.
Brace yourself
Most unpleasant and awkward situations cause us to brace ourselves. When we get stressed out, our muscles wind up around our shoulders. When we’re in pain, our muscles go up around our shoulders. We tense up and our muscles can shorten and become hypertonic.
We spend a substantial amount of time forward flexing and looking down at things all day long. We look at our phones, read and do household chores that require forward flexion. This area is constantly in flexion so when you do this you can see the appearance of wrinkles. When I take my neck and lengthen it, the skin stretches back and the appearance of lines minimizes. The jawline comes out and the bulge decreases. I think that this is area is where the treatment needs to begin.
I really started thinking outside the box at this point. There was this realization that there could be changes in the function of the structures moved by the laryngeal muscles. The neck houses some of the most important structures in our bodies that are essential to thrive, yet I have found that there is little maintenance or preventative care in these areas. It’s such a critical yet often neglected site on the body. The very first thing we do when we’re born to thrive is to breathe and eat.
When the infrahyoids and suprahyoids become tight, they pull on the hyoid and larynx. They have affect the structures they attach to. If your larynx is pulled to the side, the vocal sound changes. It directly affects sound quality. If you move the larynx out of its natural position, you will have more restrictions during swallowing.
The fine print is that these treatments do not resemble a day at the spa. They are very concentrated, they require a calm atmosphere and the recipient has to be able to tolerate the work in the front of the neck – it can be painful at times. When you are stretching muscles across their fibres, you are also stretching the nerves. Although these techniques are very safe and won’t harm the nerves, it hurts.
The treatments are modified to accommodate the tolerance levels and work safely around the structures. But every movement is very specific and slight variations are made through palpations to accommodate these differences. Your patient’s body is the guide.
I’ve had people with choking fears walk into the clinic with concerns that they are aspirating particles. After a few treatments, they are talking about how they ate their favourite pistachio ice cream or other foods with bits in them and had no troubles. Then there are the people who come in with a whisper voice and gain a voice that people in their life instantly notice – from their family to their speech pathologists.
The collection of anecdotal evidence keeps on growing and it’s exciting to think about how many people this might help.
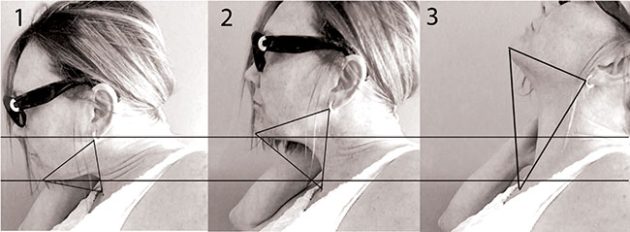
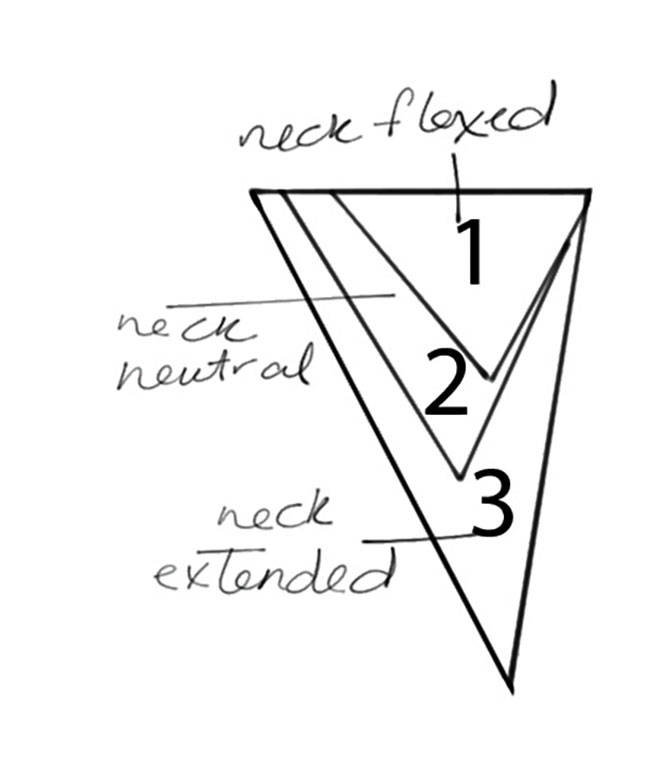
These triangles illustrate how small the space becomes in the anterior neck when head is dramatically forward flexed.
Technical tidbits
There are several structures responsible for speech and swallowing function. The less commonly discussed but highly critical structures involved with these functions are the muscles in the front of your neck, the extrinsic (outer) muscles of the larynx.
Your larynx is responsible for vocal production. Intrinsic (interior) muscles of the larynx adjust the length and tension of the vocal folds, leading to the production and quality of vocal function.
The highly flexible epiglottis is situated above the larynx. The function of the epiglottis is to cover the trachea during swallowing to prevent aspiration of food and fluids and guide them into the pharynx.
During swallowing, the hyoid bone has two muscles attached to it which act to pull it forward and upward. The other attachment site for these muscles is on the lower jaw bone (mandible). This action bulges the tongue which then presses back on the epiglottis, forcing it to close over the larynx and protect the trachea from aspiration.
If the muscles attaching to the structures attached to the epiglottis become tight and pull the larynx forward, it may compromise the inertia of the action required for a full seal of the epiglottis.
Combined with regular activities of daily living where we are flexing our heads and shoulders forward, people with Parkinson’s become increasingly forward flexed over time which decreases the space between the chin and chest. This compresses the structures in the front of the neck and you’re going to have more restrictions during swallowing.
If you were to bring your chin close to your chest, exaggerating flexion in the front of your neck and then try to speak or swallow, you should be able to feel the restrictions instantly. It does not make it impossible but certainly more challenging.
Increasing the space in the front of the neck by lengthening those muscles will take a certain amount of pressure off of the laryngeal structures. Most body systems become less efficient when they are in varying degrees of compression. The larynx is no exception.
If you move the larynx in a living body from side to side, the sound production will change, as will the ability to swallow. When there are muscle imbalances on either side, above or below the larynx, it will change the natural position of the structures. This can directly affect the optimal function of these structures. It can affect pitch, clarity and volume and ease of swallowing.
Stretching and manual manipulation intervention can be an effective way to lengthen muscles and reduce compression on the laryngeal structures.
There are many factors that affect speech and swallowing function. Not all can be improved by soft-tissue lengthening. Many instances require a SLP or the intervention of an ENT. Obtaining differential diagnosis while seeking soft tissue treatment is critical to the possible outcomes for each individual. Although, not a cure for speech and swallowing function, preventative soft tissue manipulation in early stages can help promote more optimal function and upkeep of gains.
All information collected is based on independent case studies, research and the collection of anecdotal evidence.
Cheryl Mazak is a 1996 registrant with the College of Massage Therapists of Ontario and training from the D’Arcy Lane institute. Her treatment approach is outcome-based, cross-fibre muscle lengthening techniques focused on the muscles of speech, swallowing,respiration, anterior neck and TMJ.
Print this page